
Multiple Gestation Pregnancies
Duration 10:10
Multiple Gestation Pregnancies
Liang A
Clinical Cases Applicability: Twin and higher order multiples pregnancy, IVF, TTTS
Learning Objectives:
1) Describe early fetal development from fertilization to implantation
2) Understand the physiology of twinning
3) Understand the pathophysiology of placental abnormalities in monochorionic twin pregnancies
What happens after fertilization? see figure 1
Formation of zygote (diploid cell with 46 chromosomes) in fallopian tube, day 0 cleavage to form blastomeres (cells produced by division) blastomeres divide to form a solid ball of cells known as the morula, day 3-4 accumulation of fluid between morula cells to form a blastocyst, day 4-5 (58-cell stage: 5 cells = inner cell mass, 53 outer cells = trophoblast that surrounds the ICM and the blastocele
What is “hatching”? When does the blastocyst implant?
The blastocyst is released from the zona pellucidum via secretion of proteases from the endometrium allows association of trophoblasts with endometrium for implantation at day 6-7
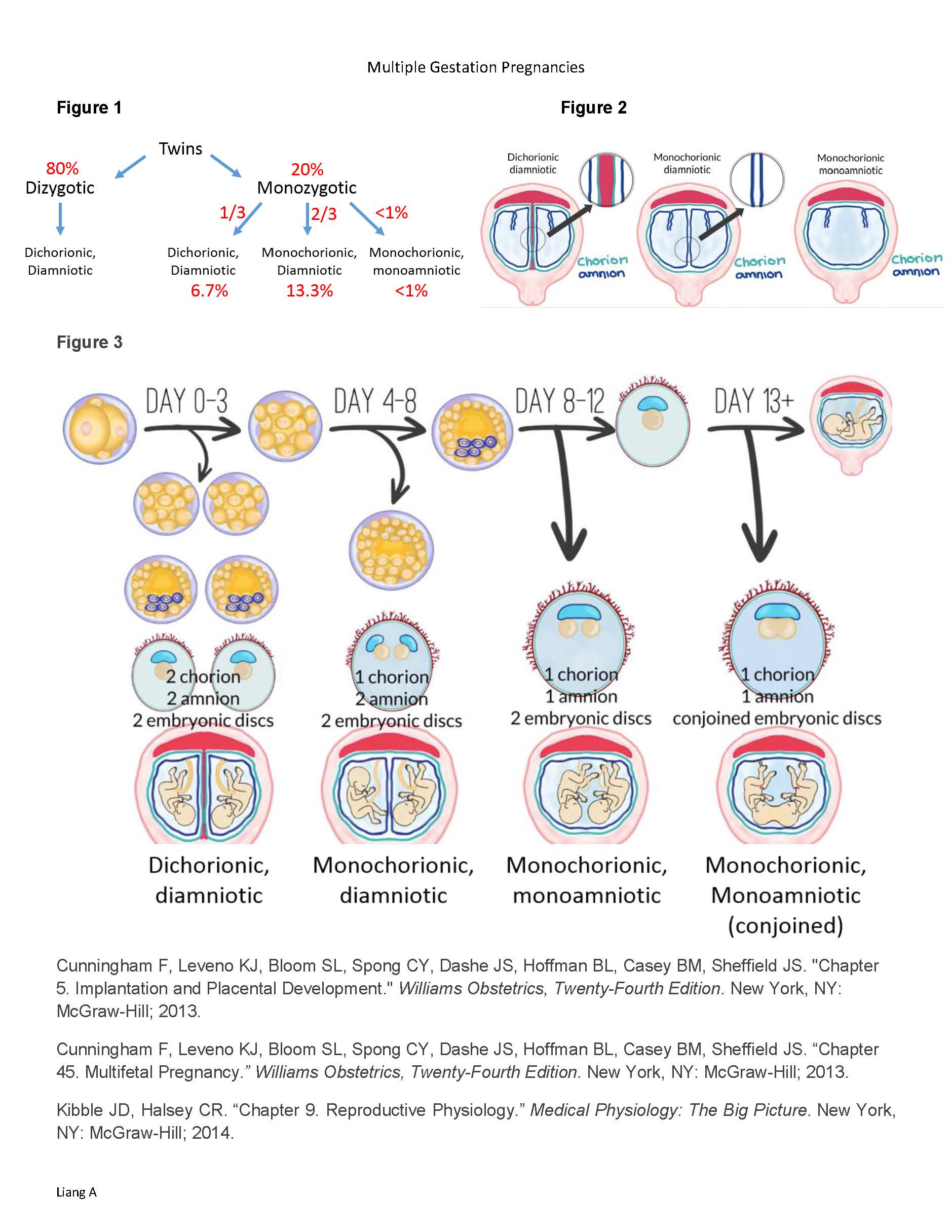
How do twins develop? Figure 1
1) 80% – Two separate ova fertilized dizygotic dichorionic, diamniotic
2) 20% – Single fertilization followed by splitting of the zygote monozygotic variable in chorionicity & # of amnion; 1/250 pregnancies – independent of race, heredity, age, parity
What determines the # of chorions and amnions in monozygotic twins? Figure 2 & 3
The timing of division
0-3 days (~33%)– di-di; before morula stage & differentiation of trophoblast
4-8 days (~67%)– mo-di; after differentiation of trophoblast, before the formation of the amnion
8-12 days (~1%)– mo-mo
>13 days – conjoined twins – mo-mo
What are common complications with multiples?
-Spontaneous abortion, congenital anomalies, hypertensive disorders, preterm delivery
-Growth restriction: Monochorionic: 1)Unequal allocation of blastomeres 2)vascular anastomoses in the placentaunequal distribution of nutrients/oxygen; Dichorionic: unequal placentation1 placental site receives more perfusion
What are unique complications of monozygotic pregnancies?
-Monoamniotic twins: high fetal death rate, estimated at 17%, >50% from cord entanglement
-Monochorionic twins: sharing fetal circulations through anastomoses of placental arteries & veins (A-A, V-V, A-V); Deep A-V communications create a “third circulation deep” within villous tissue; if significant pressure shunt develops chronic fetofetal transfusion
TTTS: Unidirectional flow through AV anastomoses – deoxygenated blood from donor placental artery pumped into a cotyledon shared by the recipient imbalance of blood volumes; Donor becomes anemic, growth restricted, oliguric with oligohydramnios (↓renal perfusion); recipient becomes polycythemic & circulatory overload (hydrops)
Treatment: laser ablation of anastomoses is preferred for severe TTTS, amnioreduction, selective feticide, septostomy (intentional creation of communication between dividing amniotic membrane) Multiple Gestation Pregnancies
Liang A
Figure 1 Figure 2
Figure 3
Cunningham F, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, Casey BM, Sheffield JS. “Chapter 5. Implantation and Placental Development.” Williams Obstetrics, Twenty-Fourth Edition. New York, NY: McGraw-Hill; 2013.
Cunningham F, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, Casey BM, Sheffield JS. “Chapter 45. Multifetal Pregnancy.” Williams Obstetrics, Twenty-Fourth Edition. New York, NY: McGraw-Hill; 2013.
Kibble JD, Halsey CR. “Chapter 9. Reproductive Physiology.” Medical Physiology: The Big Picture. New York, NY: McGraw-Hill; 2014.