
Physiology of Labor
Duration 9:46
Teaching Script: Physiology of Labor
Clinical Case Applicability:
Term Labor – normal progression to delivery vs labor dystocia
Learning Objectives:
1) Define the four phases of parturition and how they correlate to the stages of labor
2) Describe the regulation of uterine activity in pregnancy
3) Deconstruct the maternal and fetal signaling that initiate labor
4) Explain the role of oxytocin in the regulation of labor and stimulation of smooth muscle activity
Clinical Presentation:
Woman at 38 weeks gestation presents in early active labor, but labor stalls at 7 cm dilation
What is the difference between normal progression of active labor, and labor dystocia?
Review APGO videos for Educational Topics 11 and 22
• Labor – uterine contractions that cause progressive cervical effacement and dilation
• Uterine Phases of Parturition – Quiescence, Activation, Stimulation, Involution
• Labor Curve – original Friedman curve for nulliparous and multiparous patient illustrated progression of labor. Contemporary labor
practice and the consortium on safe labor describes a slower progression from 4-6 cm than the Friedman curve, and faster dilation
in multiparous patients after 6 cm than nulliparous patients.
• Labor dystocia (failed induction of labor, first or second stage arrest) may be due to factors related to the power of the uterus, the
passenger (fetus), or the passageway (maternal) which can limit the ability of the fetus to navigate the pelvis
Uterine muscle activity is constant throughout pregnancy. How is this activity regulated?
• Physiologic factors regulate the phases of parturition
• Quiescence – characterized by uterine smooth muscle relaxation with maintenance of cervical structural integrity. Inherent
myometrium contractility is suspended, and uterine muscle is primarily unresponsive to natural stimuli.
• Activation – cervical extracellular matrix changes allow progressive increases in tissue compliance or softening. Cervical softening
results from increased vascularity, stromal hypertrophy, glandular hypertrophy and hyperplasia, and slow, progressive structural
changes of the extracellular matrix. Cervical collagen undergoes conformational changes in the covalent cross-links between
proteins, that alter tissue strength and flexibility.
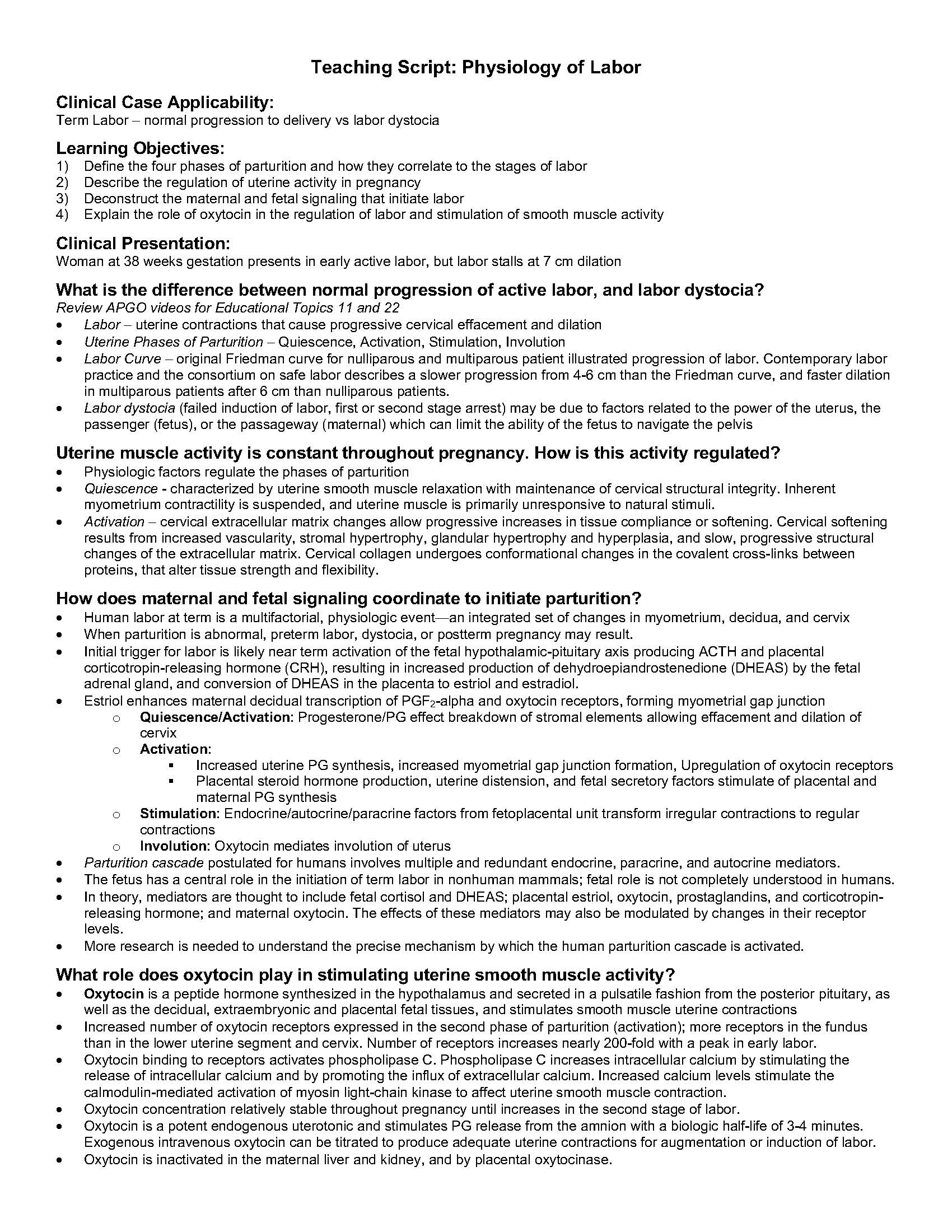
How does maternal and fetal signaling coordinate to initiate parturition?
• Human labor at term is a multifactorial, physiologic event—an integrated set of changes in myometrium, decidua, and cervix
• When parturition is abnormal, preterm labor, dystocia, or postterm pregnancy may result.
• Initial trigger for labor is likely near term activation of the fetal hypothalamic-pituitary axis producing ACTH and placental
corticotropin-releasing hormone (CRH), resulting in increased production of dehydroepiandrostenedione (DHEAS) by the fetal
adrenal gland, and conversion of DHEAS in the placenta to estriol and estradiol.
• Estriol enhances maternal decidual transcription of PGF2-alpha and oxytocin receptors, forming myometrial gap junction
o Quiescence/Activation: Progesterone/PG effect breakdown of stromal elements allowing effacement and dilation of
cervix
o Activation:
§ Increased uterine PG synthesis, increased myometrial gap junction formation, Upregulation of oxytocin receptors
§ Placental steroid hormone production, uterine distension, and fetal secretory factors stimulate of placental and
maternal PG synthesis
o Stimulation: Endocrine/autocrine/paracrine factors from fetoplacental unit transform irregular contractions to regular
contractions
o Involution: Oxytocin mediates involution of uterus
• Parturition cascade postulated for humans involves multiple and redundant endocrine, paracrine, and autocrine mediators.
• The fetus has a central role in the initiation of term labor in nonhuman mammals; fetal role is not completely understood in humans.
• In theory, mediators are thought to include fetal cortisol and DHEAS; placental estriol, oxytocin, prostaglandins, and corticotropinreleasing
hormone; and maternal oxytocin. The effects of these mediators may also be modulated by changes in their receptor
levels.
• More research is needed to understand the precise mechanism by which the human parturition cascade is activated.
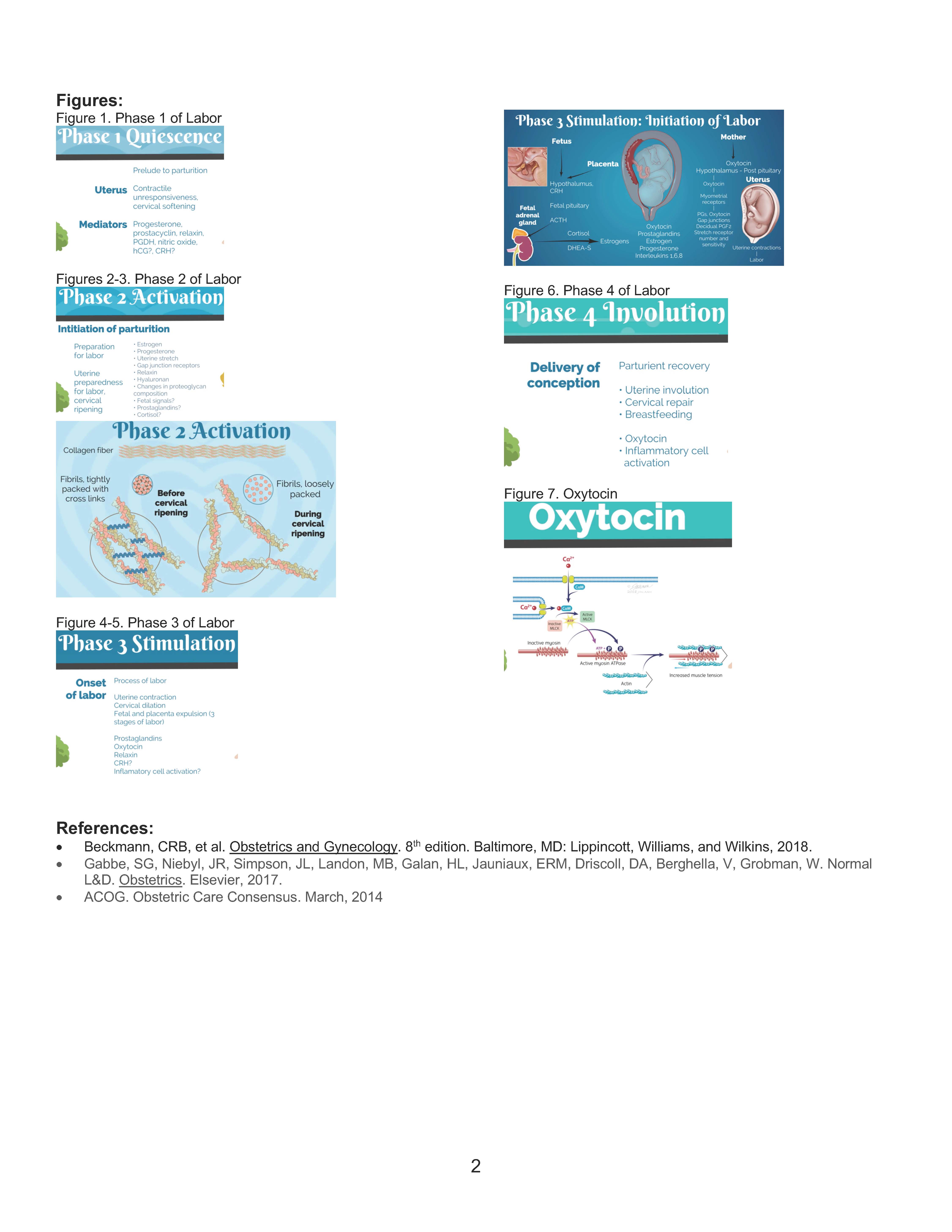
What role does oxytocin play in stimulating uterine smooth muscle activity?
• Oxytocin is a peptide hormone synthesized in the hypothalamus and secreted in a pulsatile fashion from the posterior pituitary, as
well as the decidual, extraembryonic and placental fetal tissues, and stimulates smooth muscle uterine contractions
• Increased number of oxytocin receptors expressed in the second phase of parturition (activation); more receptors in the fundus
than in the lower uterine segment and cervix. Number of receptors increases nearly 200-fold with a peak in early labor.
• Oxytocin binding to receptors activates phospholipase C. Phospholipase C increases intracellular calcium by stimulating the
release of intracellular calcium and by promoting the influx of extracellular calcium. Increased calcium levels stimulate the
calmodulin-mediated activation of myosin light-chain kinase to affect uterine smooth muscle contraction.
• Oxytocin concentration relatively stable throughout pregnancy until increases in the second stage of labor.
• Oxytocin is a potent endogenous uterotonic and stimulates PG release from the amnion with a biologic half-life of 3-4 minutes.
Exogenous intravenous oxytocin can be titrated to produce adequate uterine contractions for augmentation or induction of labor.
• Oxytocin is inactivated in the maternal liver and kidney, and by placental oxytocinase.
2
Figures:
Figure 1. Phase 1 of Labor
Figures 2-3. Phase 2 of Labor
Figure 4-5. Phase 3 of Labor
Figure 6. Phase 4 of Labor
Figure 7. Oxytocin
References:
• Beckmann, CRB, et al. Obstetrics and Gynecology. 8th edition. Baltimore, MD: Lippincott, Williams, and Wilkins, 2018.
• Gabbe, SG, Niebyl, JR, Simpson, JL, Landon, MB, Galan, HL, Jauniaux, ERM, Driscoll, DA, Berghella, V, Grobman, W. Normal
L&D. Obstetrics. Elsevier, 2017.
• ACOG. Obstetric Care Consensus. March, 2014