
Alloimmunization
Duration 8:54
Teaching Script: Alloimmunization
Clinical Case Applicability:
Prenatal diagnosis – Fetal hydrops, In utero fetal demise or spontaneous abortion, Antepartum care, Fetal-maternal hemorrhage
Learning Objectives:
1) Describe the role of fetal hematopoiesis and the genetics of common red cell membrane antigens
2) Recognize the clinically relevant red cell antigens associated with alloimmunization
3) Describe the pathogenesis of fetal hemolytic anemia due to alloimmunization
4) Explain how to assess fetal risk and diagnose red cell alloimmunization
5) Summarize the possible mechanism(s) by which Rh-immunoglobulin is thought to prevent future alloimmunization
Clinical Presentation:
Miscarriage (prevention); Third trimester demise of hydropic fetus
When and where does fetal hematopoiesis occur during gestation?
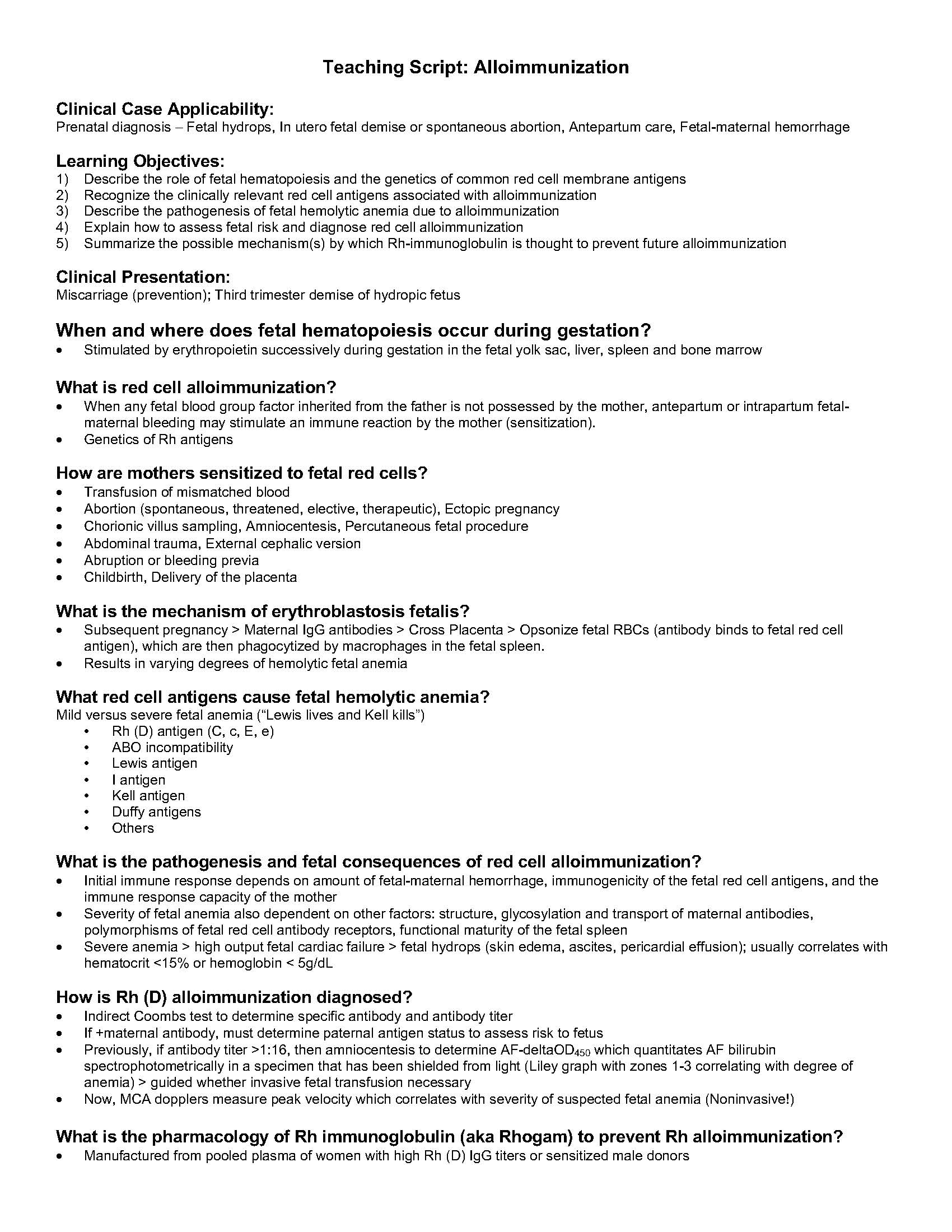
• Stimulated by erythropoietin successively during gestation in the fetal yolk sac, liver, spleen and bone marrow
What is red cell alloimmunization?
• When any fetal blood group factor inherited from the father is not possessed by the mother, antepartum or intrapartum fetalmaternal
bleeding may stimulate an immune reaction by the mother (sensitization).
• Genetics of Rh antigens
How are mothers sensitized to fetal red cells?
• Transfusion of mismatched blood
• Abortion (spontaneous, threatened, elective, therapeutic), Ectopic pregnancy
• Chorionic villus sampling, Amniocentesis, Percutaneous fetal procedure
• Abdominal trauma, External cephalic version
• Abruption or bleeding previa
• Childbirth, Delivery of the placenta
What is the mechanism of erythroblastosis fetalis?
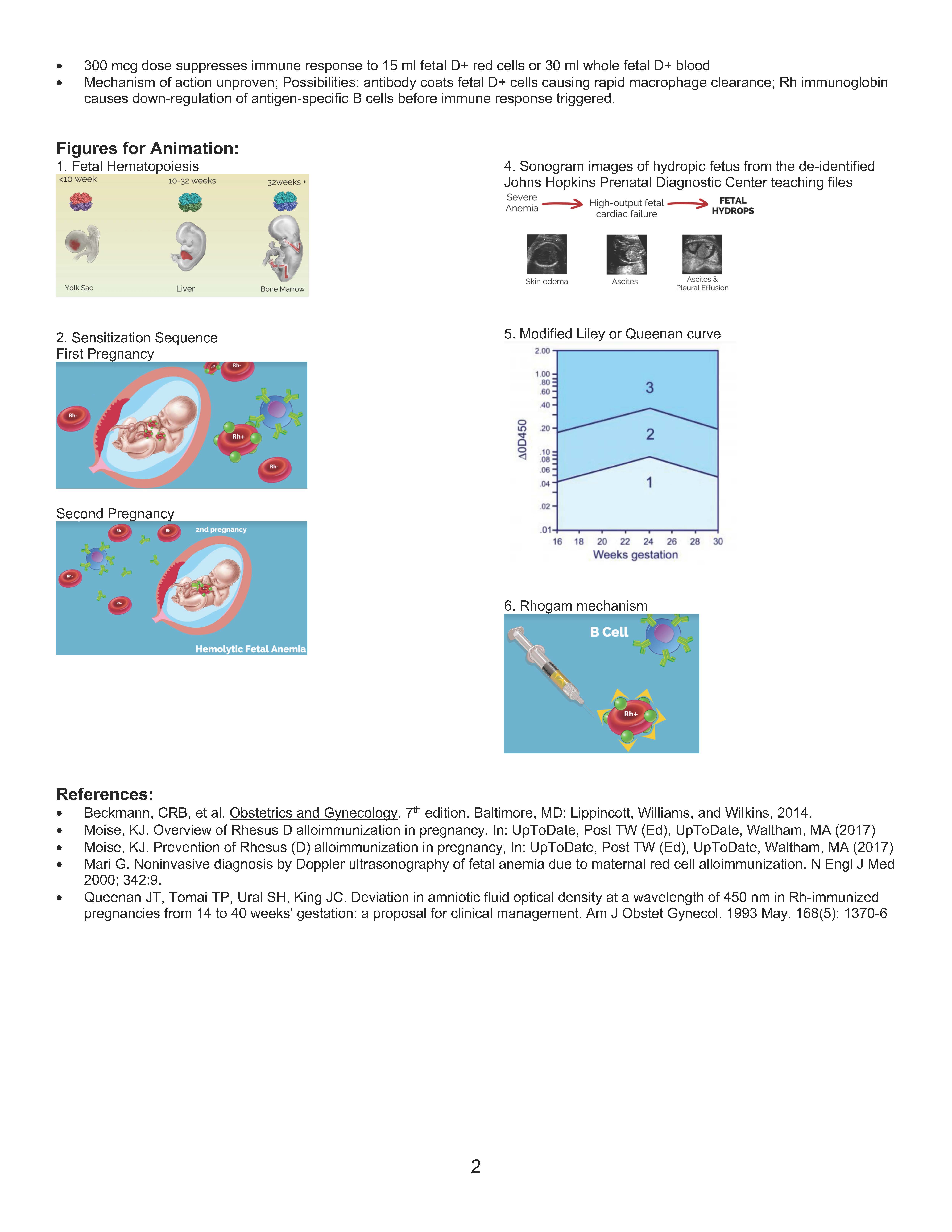
• Subsequent pregnancy > Maternal IgG antibodies > Cross Placenta > Opsonize fetal RBCs (antibody binds to fetal red cell
antigen), which are then phagocytized by macrophages in the fetal spleen.
• Results in varying degrees of hemolytic fetal anemia
What red cell antigens cause fetal hemolytic anemia?
Mild versus severe fetal anemia (“Lewis lives and Kell kills”)
• Rh (D) antigen (C, c, E, e)
• ABO incompatibility
• Lewis antigen
• I antigen
• Kell antigen
• Duffy antigens
• Others
What is the pathogenesis and fetal consequences of red cell alloimmunization?
• Initial immune response depends on amount of fetal-maternal hemorrhage, immunogenicity of the fetal red cell antigens, and the
immune response capacity of the mother
• Severity of fetal anemia also dependent on other factors: structure, glycosylation and transport of maternal antibodies,
polymorphisms of fetal red cell antibody receptors, functional maturity of the fetal spleen
• Severe anemia > high output fetal cardiac failure > fetal hydrops (skin edema, ascites, pericardial effusion); usually correlates with
hematocrit <15% or hemoglobin < 5g/dL
How is Rh (D) alloimmunization diagnosed?
• Indirect Coombs test to determine specific antibody and antibody titer
• If +maternal antibody, must determine paternal antigen status to assess risk to fetus
• Previously, if antibody titer >1:16, then amniocentesis to determine AF-deltaOD450 which quantitates AF bilirubin
spectrophotometrically in a specimen that has been shielded from light (Liley graph with zones 1-3 correlating with degree of
anemia) > guided whether invasive fetal transfusion necessary
• Now, MCA dopplers measure peak velocity which correlates with severity of suspected fetal anemia (Noninvasive!)
What is the pharmacology of Rh immunoglobulin (aka Rhogam) to prevent Rh alloimmunization?
• Manufactured from pooled plasma of women with high Rh (D) IgG titers or sensitized male donors
2
• 300 mcg dose suppresses immune response to 15 ml fetal D+ red cells or 30 ml whole fetal D+ blood
• Mechanism of action unproven; Possibilities: antibody coats fetal D+ cells causing rapid macrophage clearance; Rh immunoglobin
causes down-regulation of antigen-specific B cells before immune response triggered.
Figures for Animation:
1. Fetal Hematopoiesis
2. Sensitization Sequence
First Pregnancy
Second Pregnancy
4. Sonogram images of hydropic fetus from the de-identified
Johns Hopkins Prenatal Diagnostic Center teaching files
5. Modified Liley or Queenan curve
6. Rhogam mechanism
References:
• Beckmann, CRB, et al. Obstetrics and Gynecology. 7th edition. Baltimore, MD: Lippincott, Williams, and Wilkins, 2014.
• Moise, KJ. Overview of Rhesus D alloimmunization in pregnancy. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA (2017)
• Moise, KJ. Prevention of Rhesus (D) alloimmunization in pregnancy, In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA (2017)
• Mari G. Noninvasive diagnosis by Doppler ultrasonography of fetal anemia due to maternal red cell alloimmunization. N Engl J Med
2000; 342:9.
• Queenan JT, Tomai TP, Ural SH, King JC. Deviation in amniotic fluid optical density at a wavelength of 450 nm in Rh-immunized
pregnancies from 14 to 40 weeks’ gestation: a proposal for clinical management. Am J Obstet Gynecol. 1993 May. 168(5): 1370-6