
Aneuploidy Screening
Duration 8:38
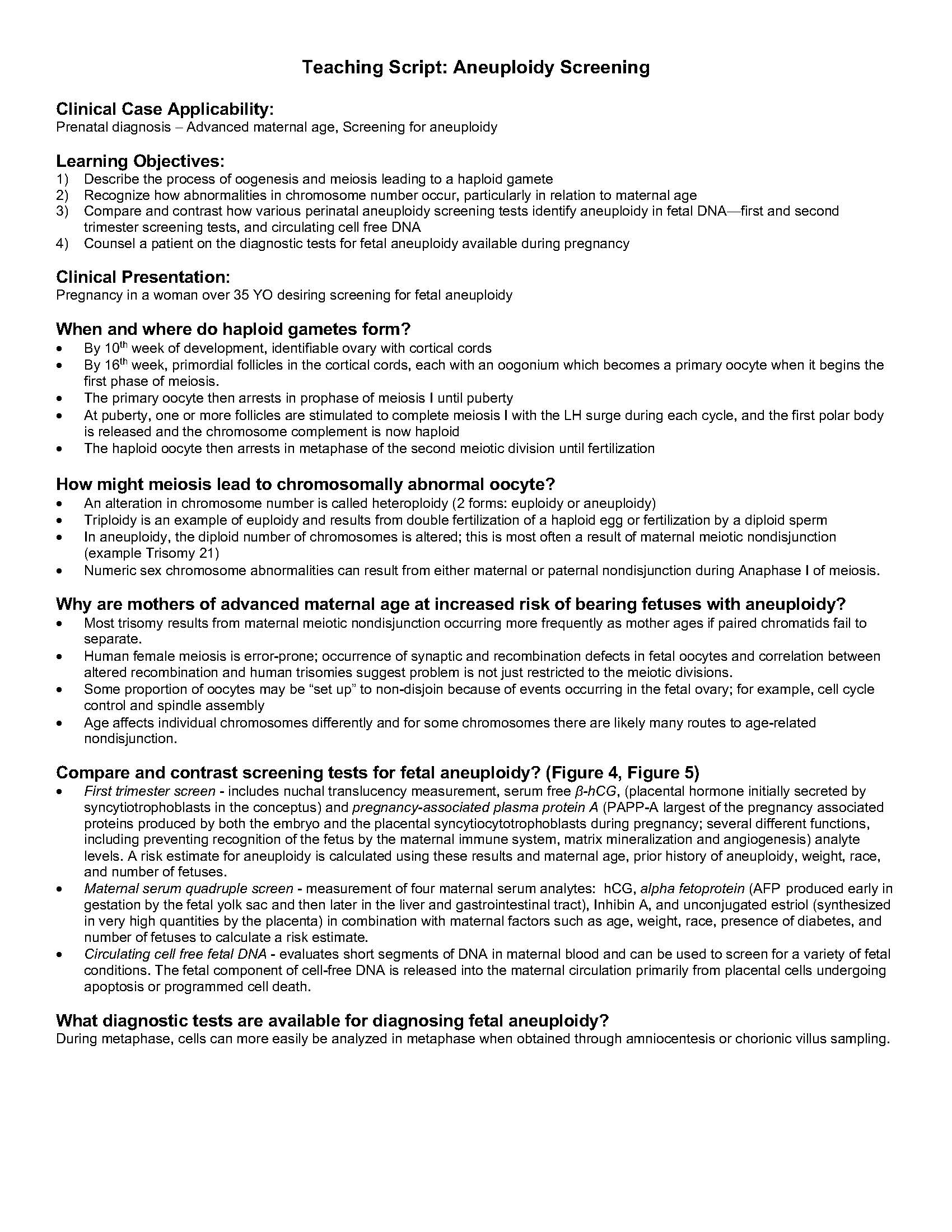
Teaching Script: Aneuploidy Screening
Clinical Case Applicability:
Prenatal diagnosis – Advanced maternal age, Screening for aneuploidy
Learning Objectives:
1) Describe the process of oogenesis and meiosis leading to a haploid gamete
2) Recognize how abnormalities in chromosome number occur, particularly in relation to maternal age
3) Compare and contrast how various perinatal aneuploidy screening tests identify aneuploidy in fetal DNA—first and second
trimester screening tests, and circulating cell free DNA
4) Counsel a patient on the diagnostic tests for fetal aneuploidy available during pregnancy
Clinical Presentation:
Pregnancy in a woman over 35 YO desiring screening for fetal aneuploidy
When and where do haploid gametes form?
• By 10th week of development, identifiable ovary with cortical cords
• By 16th week, primordial follicles in the cortical cords, each with an oogonium which becomes a primary oocyte when it begins the
first phase of meiosis.
• The primary oocyte then arrests in prophase of meiosis I until puberty
• At puberty, one or more follicles are stimulated to complete meiosis I with the LH surge during each cycle, and the first polar body
is released and the chromosome complement is now haploid
• The haploid oocyte then arrests in metaphase of the second meiotic division until fertilization
How might meiosis lead to chromosomally abnormal oocyte?
• An alteration in chromosome number is called heteroploidy (2 forms: euploidy or aneuploidy)
• Triploidy is an example of euploidy and results from double fertilization of a haploid egg or fertilization by a diploid sperm
• In aneuploidy, the diploid number of chromosomes is altered; this is most often a result of maternal meiotic nondisjunction
(example Trisomy 21)
• Numeric sex chromosome abnormalities can result from either maternal or paternal nondisjunction during Anaphase I of meiosis.
Why are mothers of advanced maternal age at increased risk of bearing fetuses with aneuploidy?
• Most trisomy results from maternal meiotic nondisjunction occurring more frequently as mother ages if paired chromatids fail to
separate.
• Human female meiosis is error-prone; occurrence of synaptic and recombination defects in fetal oocytes and correlation between
altered recombination and human trisomies suggest problem is not just restricted to the meiotic divisions.
• Some proportion of oocytes may be “set up” to non-disjoin because of events occurring in the fetal ovary; for example, cell cycle
control and spindle assembly
• Age affects individual chromosomes differently and for some chromosomes there are likely many routes to age-related
nondisjunction.
Compare and contrast screening tests for fetal aneuploidy? (Figure 4, Figure 5)
• First trimester screen – includes nuchal translucency measurement, serum free β-hCG, (placental hormone initially secreted by
syncytiotrophoblasts in the conceptus) and pregnancy-associated plasma protein A (PAPP-A largest of the pregnancy associated
proteins produced by both the embryo and the placental syncytiocytotrophoblasts during pregnancy; several different functions,
including preventing recognition of the fetus by the maternal immune system, matrix mineralization and angiogenesis) analyte
levels. A risk estimate for aneuploidy is calculated using these results and maternal age, prior history of aneuploidy, weight, race,
and number of fetuses.
• Maternal serum quadruple screen – measurement of four maternal serum analytes: hCG, alpha fetoprotein (AFP produced early in
gestation by the fetal yolk sac and then later in the liver and gastrointestinal tract), Inhibin A, and unconjugated estriol (synthesized
in very high quantities by the placenta) in combination with maternal factors such as age, weight, race, presence of diabetes, and
number of fetuses to calculate a risk estimate.
• Circulating cell free fetal DNA – evaluates short segments of DNA in maternal blood and can be used to screen for a variety of fetal
conditions. The fetal component of cell-free DNA is released into the maternal circulation primarily from placental cells undergoing
apoptosis or programmed cell death.
What diagnostic tests are available for diagnosing fetal aneuploidy?
During metaphase, cells can more easily be analyzed in metaphase when obtained through amniocentesis or chorionic villus sampling.
2
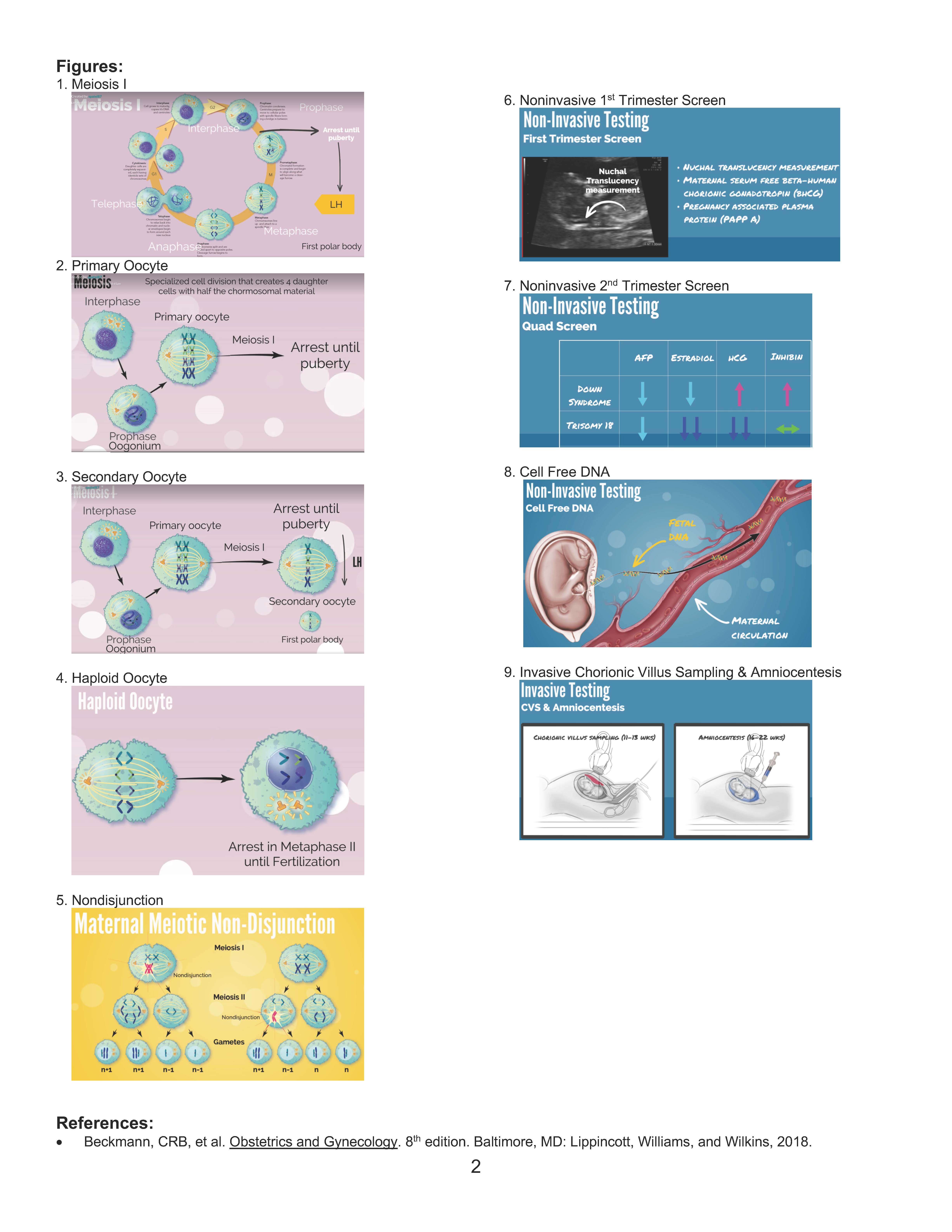
Figures:
1. Meiosis I
2. Primary Oocyte
3. Secondary Oocyte
4. Haploid Oocyte
5. Nondisjunction
6. Noninvasive 1st Trimester Screen
7. Noninvasive 2nd Trimester Screen
8. Cell Free DNA
9. Invasive Chorionic Villus Sampling & Amniocentesis
References:
• Beckmann, CRB, et al. Obstetrics and Gynecology. 8th edition. Baltimore, MD: Lippincott, Williams, and Wilkins, 2018.