
Breast Disorders
Duration 11:24
Disorders of the Breast
Liang A
Clinical case applicability: Breast mass/discharge, screening mammography, breast cancer
Learning Objectives:
1. Understand normal breast anatomy and histology
2. Identify common breast disorders & breast cancer
3. Understand the mechanism of action for hormonal therapies for breast cancer
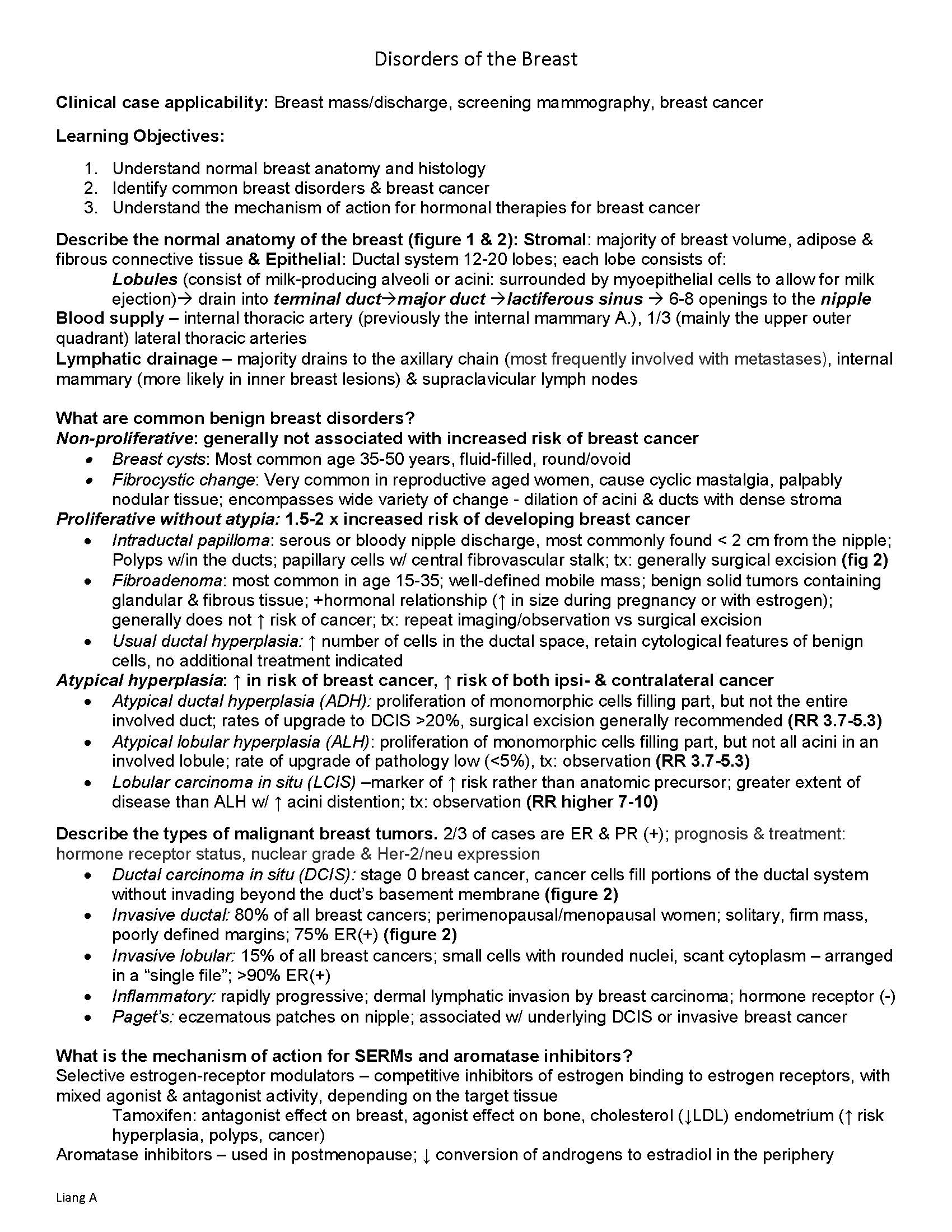
Describe the normal anatomy of the breast (figure 1 & 2): Stromal: majority of breast volume, adipose & fibrous connective tissue & Epithelial: Ductal system 12-20 lobes; each lobe consists of:
Lobules (consist of milk-producing alveoli or acini: surrounded by myoepithelial cells to allow for milk ejection) drain into terminal ductmajor duct lactiferous sinus 6-8 openings to the nipple
Blood supply – internal thoracic artery (previously the internal mammary A.), 1/3 (mainly the upper outer quadrant) lateral thoracic arteries
Lymphatic drainage – majority drains to the axillary chain (most frequently involved with metastases), internal mammary (more likely in inner breast lesions) & supraclavicular lymph nodes
What are common benign breast disorders?
Non-proliferative: generally not associated with increased risk of breast cancer
Breast cysts: Most common age 35-50 years, fluid-filled, round/ovoid
Fibrocystic change: Very common in reproductive aged women, cause cyclic mastalgia, palpably nodular tissue; encompasses wide variety of change – dilation of acini & ducts with dense stroma
Proliferative without atypia: 1.5-2 x increased risk of developing breast cancer
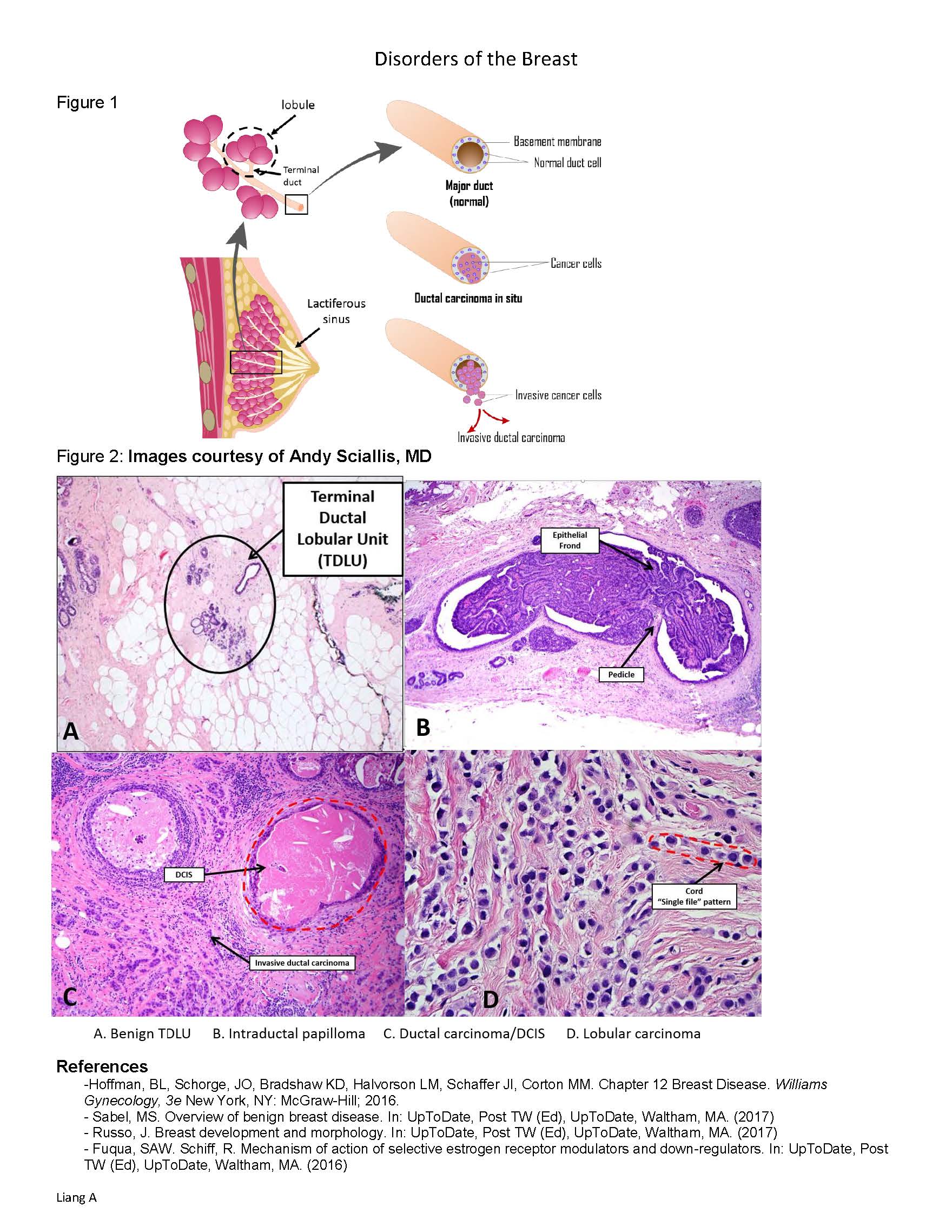
Intraductal papilloma: serous or bloody nipple discharge, most commonly found < 2 cm from the nipple; Polyps w/in the ducts; papillary cells w/ central fibrovascular stalk; tx: generally surgical excision (fig 2)
Fibroadenoma: most common in age 15-35; well-defined mobile mass; benign solid tumors containing glandular & fibrous tissue; +hormonal relationship (↑ in size during pregnancy or with estrogen); generally does not ↑ risk of cancer; tx: repeat imaging/observation vs surgical excision
Usual ductal hyperplasia: ↑ number of cells in the ductal space, retain cytological features of benign cells, no additional treatment indicated
Atypical hyperplasia: ↑ in risk of breast cancer, ↑ risk of both ipsi- & contralateral cancer
Atypical ductal hyperplasia (ADH): proliferation of monomorphic cells filling part, but not the entire involved duct; rates of upgrade to DCIS >20%, surgical excision generally recommended (RR 3.7-5.3)
Atypical lobular hyperplasia (ALH): proliferation of monomorphic cells filling part, but not all acini in an involved lobule; rate of upgrade of pathology low (<5%), tx: observation (RR 3.7-5.3)
Lobular carcinoma in situ (LCIS) –marker of ↑ risk rather than anatomic precursor; greater extent of disease than ALH w/ ↑ acini distention; tx: observation (RR higher 7-10)
Describe the types of malignant breast tumors. 2/3 of cases are ER & PR (+); prognosis & treatment: hormone receptor status, nuclear grade & Her-2/neu expression
Ductal carcinoma in situ (DCIS): stage 0 breast cancer, cancer cells fill portions of the ductal system without invading beyond the duct’s basement membrane (figure 2)
Invasive ductal: 80% of all breast cancers; perimenopausal/menopausal women; solitary, firm mass, poorly defined margins; 75% ER(+) (figure 2)
Invasive lobular: 15% of all breast cancers; small cells with rounded nuclei, scant cytoplasm – arranged in a “single file”; >90% ER(+)
Inflammatory: rapidly progressive; dermal lymphatic invasion by breast carcinoma; hormone receptor (-)
Paget’s: eczematous patches on nipple; associated w/ underlying DCIS or invasive breast cancer
What is the mechanism of action for SERMs and aromatase inhibitors?
Selective estrogen-receptor modulators – competitive inhibitors of estrogen binding to estrogen receptors, with mixed agonist & antagonist activity, depending on the target tissue
Tamoxifen: antagonist effect on breast, agonist effect on bone, cholesterol (↓LDL) endometrium (↑ risk hyperplasia, polyps, cancer)
Aromatase inhibitors – used in postmenopause; ↓ conversion of androgens to estradiol in the periphery Disorders of the Breast
Liang A
Figure 1
Figure 2: Images courtesy of Andy Sciallis, MD
References
-Hoffman, BL, Schorge, JO, Bradshaw KD, Halvorson LM, Schaffer JI, Corton MM. Chapter 12 Breast Disease. Williams Gynecology, 3e New York, NY: McGraw-Hill; 2016.
– Sabel, MS. Overview of benign breast disease. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (2017)
– Russo, J. Breast development and morphology. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (2017)
– Fuqua, SAW. Schiff, R. Mechanism of action of selective estrogen receptor modulators and down-regulators. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (2016)