
Embryology of Common Malformations
Duration 14:50
Teaching Script: Embryology of Common Malformations
Clinical Case Applicability:
Prenatal diagnosis – First trimester ultrasound, Second trimester anatomy screen; Preconception consultation
Learning Objectives:
1) Describe the development of the embryo and germ layers – ectoderm, mesoderm, endoderm
2) Understand the critical periods in embryogenesis and how these correlates with the development of particular malformations
3) Define the terms describing congenital anomalies and patterns of malformations
4) Identify the factors that affect embryogenesis and the mechanisms that alter normal embryogenesis
Clinical Presentation:
Pregnancy in a 26 YO woman with poorly controlled diabetes preconceptionally or with seizure disorder on valproate
Review the development of the embryonic germ layers after conception.
• Week 1: Following fertilization, the embryo begins to divide: 2 cell (Day 2), Morula (Day 3), and Early Blastocyst (Day 4)
o Blastocyst – Cells segregate into inner cell mass (embryoblast) and outer cell mass (trophoblast)
o Trophoblast contributes to the placenta and begins implantation
• Week 2: Blastocyst is partially embedded in the endometrium
o Trophoblast differentiates into the cytotrophoblast and syncytiotrophoblast
o Embryoblast forms bilaminar disc – epiblast and hypoblast
o Extraembryonic mesoderm splits into somatic and splanchnic layers
o Two cavities are formed – amniotic sac and yolk sac
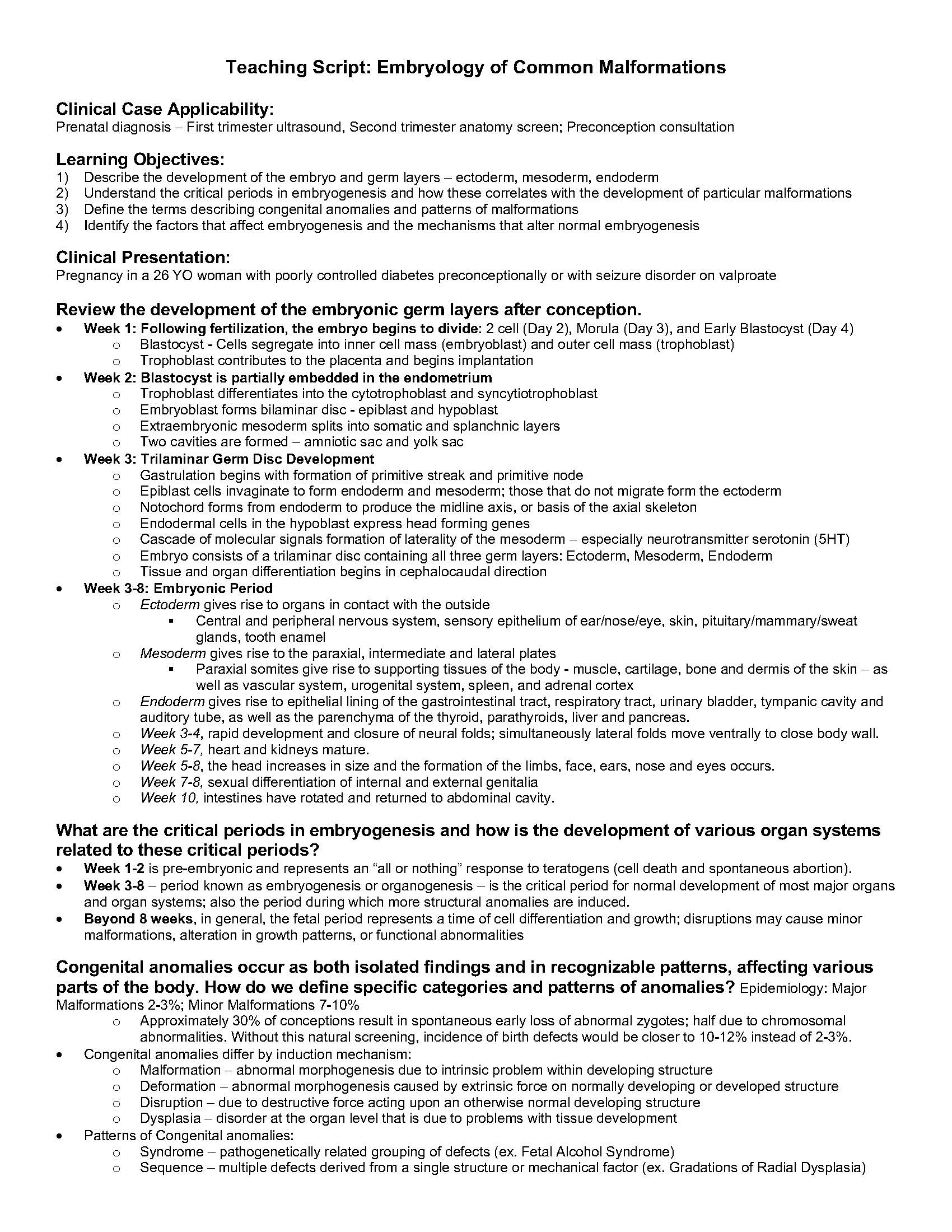
• Week 3: Trilaminar Germ Disc Development
o Gastrulation begins with formation of primitive streak and primitive node
o Epiblast cells invaginate to form endoderm and mesoderm; those that do not migrate form the ectoderm
o Notochord forms from endoderm to produce the midline axis, or basis of the axial skeleton
o Endodermal cells in the hypoblast express head forming genes
o Cascade of molecular signals formation of laterality of the mesoderm – especially neurotransmitter serotonin (5HT)
o Embryo consists of a trilaminar disc containing all three germ layers: Ectoderm, Mesoderm, Endoderm
o Tissue and organ differentiation begins in cephalocaudal direction
• Week 3-8: Embryonic Period
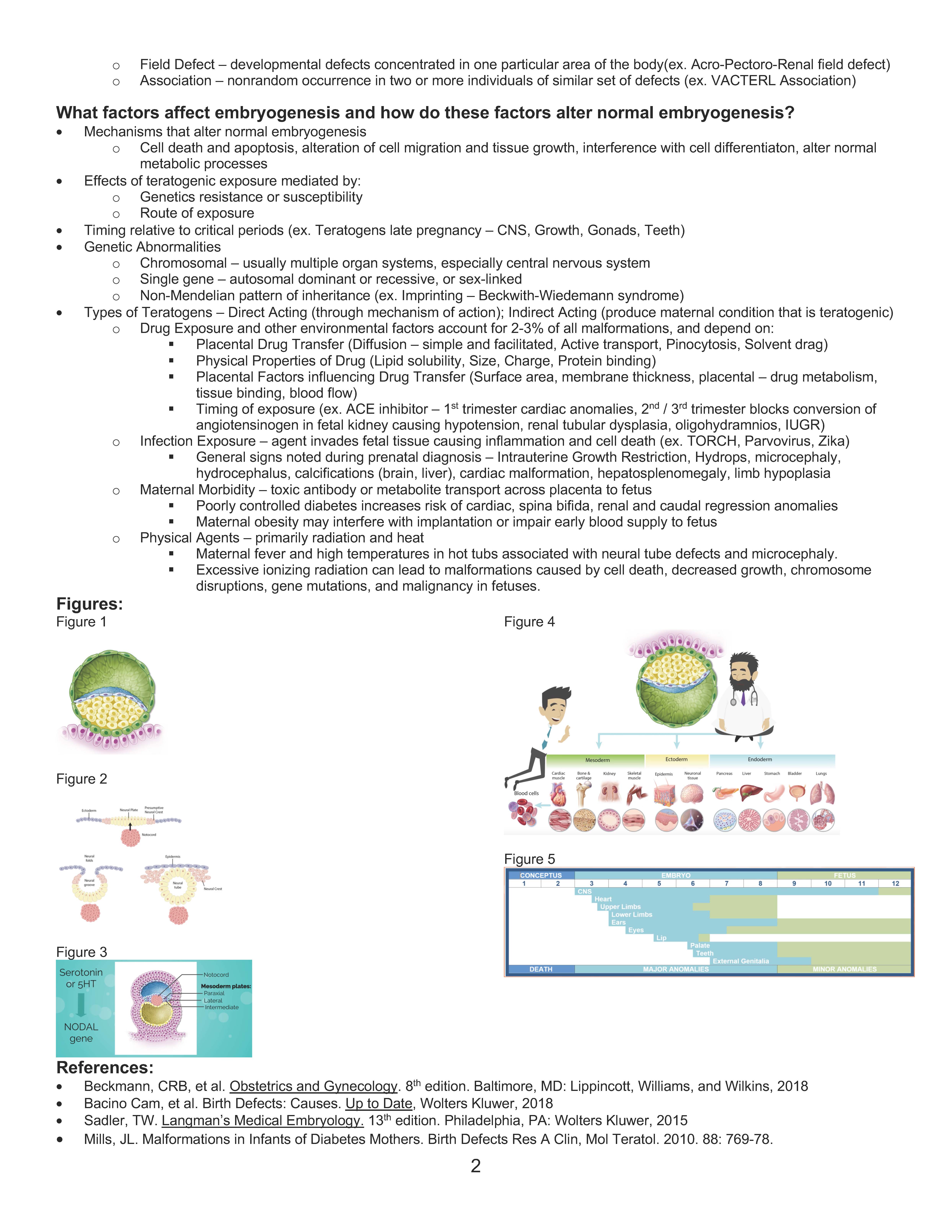
o Ectoderm gives rise to organs in contact with the outside
§ Central and peripheral nervous system, sensory epithelium of ear/nose/eye, skin, pituitary/mammary/sweat
glands, tooth enamel
o Mesoderm gives rise to the paraxial, intermediate and lateral plates
§ Paraxial somites give rise to supporting tissues of the body – muscle, cartilage, bone and dermis of the skin – as
well as vascular system, urogenital system, spleen, and adrenal cortex
o Endoderm gives rise to epithelial lining of the gastrointestinal tract, respiratory tract, urinary bladder, tympanic cavity and
auditory tube, as well as the parenchyma of the thyroid, parathyroids, liver and pancreas.
o Week 3-4, rapid development and closure of neural folds; simultaneously lateral folds move ventrally to close body wall.
o Week 5-7, heart and kidneys mature.
o Week 5-8, the head increases in size and the formation of the limbs, face, ears, nose and eyes occurs.
o Week 7-8, sexual differentiation of internal and external genitalia
o Week 10, intestines have rotated and returned to abdominal cavity.
What are the critical periods in embryogenesis and how is the development of various organ systems
related to these critical periods?
• Week 1-2 is pre-embryonic and represents an “all or nothing” response to teratogens (cell death and spontaneous abortion).
• Week 3-8 – period known as embryogenesis or organogenesis – is the critical period for normal development of most major organs
and organ systems; also the period during which more structural anomalies are induced.
• Beyond 8 weeks, in general, the fetal period represents a time of cell differentiation and growth; disruptions may cause minor
malformations, alteration in growth patterns, or functional abnormalities
Congenital anomalies occur as both isolated findings and in recognizable patterns, affecting various
parts of the body. How do we define specific categories and patterns of anomalies? Epidemiology: Major
Malformations 2-3%; Minor Malformations 7-10%
o Approximately 30% of conceptions result in spontaneous early loss of abnormal zygotes; half due to chromosomal
abnormalities. Without this natural screening, incidence of birth defects would be closer to 10-12% instead of 2-3%.
• Congenital anomalies differ by induction mechanism:
o Malformation – abnormal morphogenesis due to intrinsic problem within developing structure
o Deformation – abnormal morphogenesis caused by extrinsic force on normally developing or developed structure
o Disruption – due to destructive force acting upon an otherwise normal developing structure
o Dysplasia – disorder at the organ level that is due to problems with tissue development
• Patterns of Congenital anomalies:
o Syndrome – pathogenetically related grouping of defects (ex. Fetal Alcohol Syndrome)
o Sequence – multiple defects derived from a single structure or mechanical factor (ex. Gradations of Radial Dysplasia)
2
o Field Defect – developmental defects concentrated in one particular area of the body(ex. Acro-Pectoro-Renal field defect)
o Association – nonrandom occurrence in two or more individuals of similar set of defects (ex. VACTERL Association)
What factors affect embryogenesis and how do these factors alter normal embryogenesis?
• Mechanisms that alter normal embryogenesis
o Cell death and apoptosis, alteration of cell migration and tissue growth, interference with cell differentiaton, alter normal
metabolic processes
• Effects of teratogenic exposure mediated by:
o Genetics resistance or susceptibility
o Route of exposure
• Timing relative to critical periods (ex. Teratogens late pregnancy – CNS, Growth, Gonads, Teeth)
• Genetic Abnormalities
o Chromosomal – usually multiple organ systems, especially central nervous system
o Single gene – autosomal dominant or recessive, or sex-linked
o Non-Mendelian pattern of inheritance (ex. Imprinting – Beckwith-Wiedemann syndrome)
• Types of Teratogens – Direct Acting (through mechanism of action); Indirect Acting (produce maternal condition that is teratogenic)
o Drug Exposure and other environmental factors account for 2-3% of all malformations, and depend on:
§ Placental Drug Transfer (Diffusion – simple and facilitated, Active transport, Pinocytosis, Solvent drag)
§ Physical Properties of Drug (Lipid solubility, Size, Charge, Protein binding)
§ Placental Factors influencing Drug Transfer (Surface area, membrane thickness, placental – drug metabolism,
tissue binding, blood flow)
§ Timing of exposure (ex. ACE inhibitor – 1st trimester cardiac anomalies, 2nd / 3rd trimester blocks conversion of
angiotensinogen in fetal kidney causing hypotension, renal tubular dysplasia, oligohydramnios, IUGR)
o Infection Exposure – agent invades fetal tissue causing inflammation and cell death (ex. TORCH, Parvovirus, Zika)
§ General signs noted during prenatal diagnosis – Intrauterine Growth Restriction, Hydrops, microcephaly,
hydrocephalus, calcifications (brain, liver), cardiac malformation, hepatosplenomegaly, limb hypoplasia
o Maternal Morbidity – toxic antibody or metabolite transport across placenta to fetus
§ Poorly controlled diabetes increases risk of cardiac, spina bifida, renal and caudal regression anomalies
§ Maternal obesity may interfere with implantation or impair early blood supply to fetus
o Physical Agents – primarily radiation and heat
§ Maternal fever and high temperatures in hot tubs associated with neural tube defects and microcephaly.
§ Excessive ionizing radiation can lead to malformations caused by cell death, decreased growth, chromosome
disruptions, gene mutations, and malignancy in fetuses.
Figures:
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
References:
• Beckmann, CRB, et al. Obstetrics and Gynecology. 8th edition. Baltimore, MD: Lippincott, Williams, and Wilkins, 2018
• Bacino Cam, et al. Birth Defects: Causes. Up to Date, Wolters Kluwer, 2018
• Sadler, TW. Langman’s Medical Embryology. 13th edition. Philadelphia, PA: Wolters Kluwer, 2015
• Mills, JL. Malformations in Infants of Diabetes Mothers. Birth Defects Res A Clin, Mol Teratol. 2010. 88: 769-78.