
Gestational Diabetes
Duration 11:43
Teaching Script: Gestational Diabetes
Clinical Case Applicability:
Gestational diabetes, History of fetal macrosomia
Learning Objectives:
1) Review the risk factors for gestational diabetes mellitus (GDM)
2) Describe glucose metabolism relative to normal maternal physiology adaptation in pregnancy
3) Understand the pathophysiology of impaired glucose metabolism in GDM
4) Outline the approach to screening and diagnosis of GDM
5) Understand how altered glucose metabolism in GDM can affect the fetus
6) Identify and describe the mechanism of action, pharmacokinetics, and therapeutic use of hypoglycemic agents used to treat GDM
Clinical Presentation:
Pregnancy in a woman over 35 YO at 32 weeks gestation with 40lb pregnancy weight gain and positive screen for GDM
What risk factors are associated with development of GDM?
• GDM is defined as carbohydrate intolerance with onset during pregnancy
o A1 = Diet controlled
o A2 = Not diet controlled
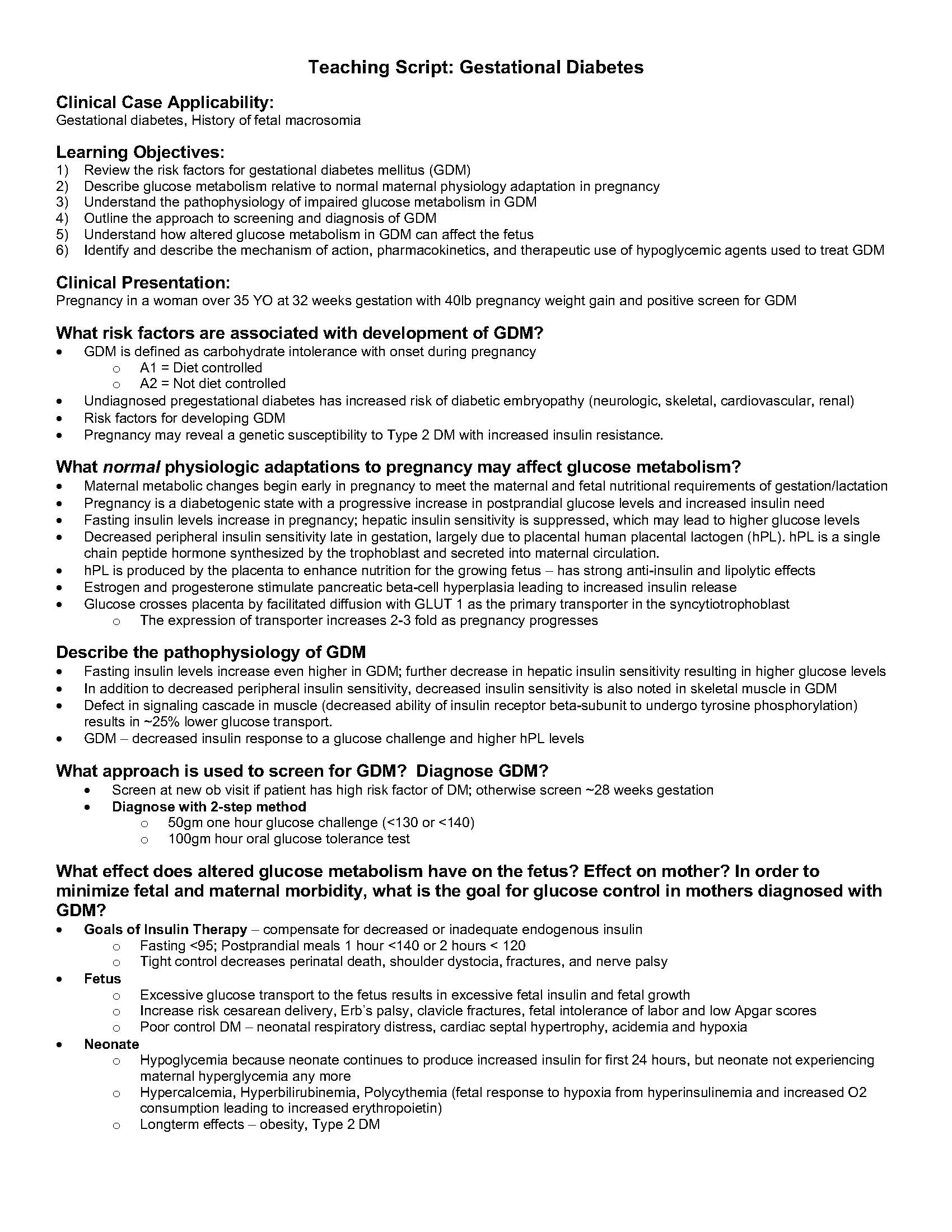
• Undiagnosed pregestational diabetes has increased risk of diabetic embryopathy (neurologic, skeletal, cardiovascular, renal)
• Risk factors for developing GDM
• Pregnancy may reveal a genetic susceptibility to Type 2 DM with increased insulin resistance.
What normal physiologic adaptations to pregnancy may affect glucose metabolism?
• Maternal metabolic changes begin early in pregnancy to meet the maternal and fetal nutritional requirements of gestation/lactation
• Pregnancy is a diabetogenic state with a progressive increase in postprandial glucose levels and increased insulin need
• Fasting insulin levels increase in pregnancy; hepatic insulin sensitivity is suppressed, which may lead to higher glucose levels
• Decreased peripheral insulin sensitivity late in gestation, largely due to placental human placental lactogen (hPL). hPL is a single
chain peptide hormone synthesized by the trophoblast and secreted into maternal circulation.
• hPL is produced by the placenta to enhance nutrition for the growing fetus – has strong anti-insulin and lipolytic effects
• Estrogen and progesterone stimulate pancreatic beta-cell hyperplasia leading to increased insulin release
• Glucose crosses placenta by facilitated diffusion with GLUT 1 as the primary transporter in the syncytiotrophoblast
o The expression of transporter increases 2-3 fold as pregnancy progresses
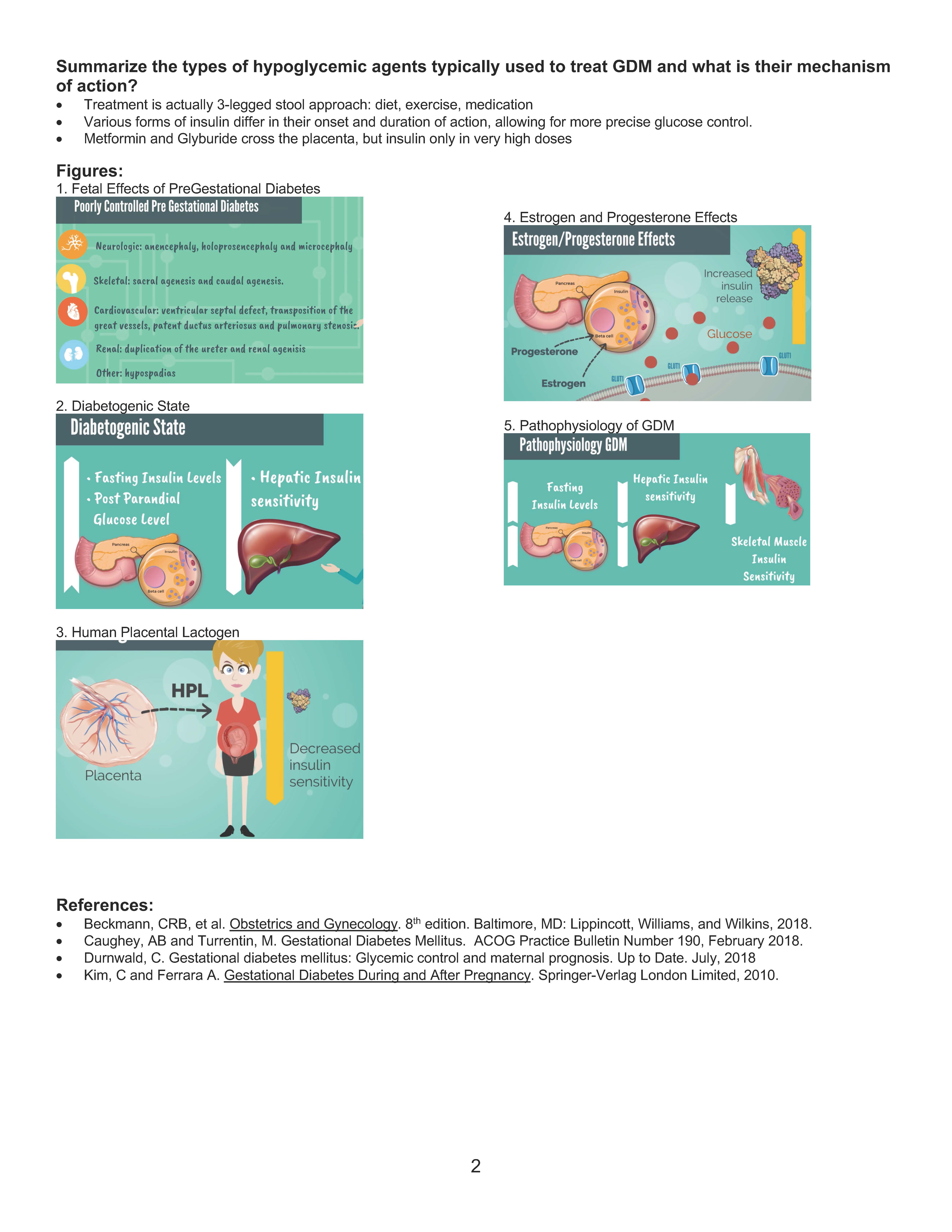
Describe the pathophysiology of GDM
• Fasting insulin levels increase even higher in GDM; further decrease in hepatic insulin sensitivity resulting in higher glucose levels
• In addition to decreased peripheral insulin sensitivity, decreased insulin sensitivity is also noted in skeletal muscle in GDM
• Defect in signaling cascade in muscle (decreased ability of insulin receptor beta-subunit to undergo tyrosine phosphorylation)
results in ~25% lower glucose transport.
• GDM – decreased insulin response to a glucose challenge and higher hPL levels
What approach is used to screen for GDM? Diagnose GDM?
• Screen at new ob visit if patient has high risk factor of DM; otherwise screen ~28 weeks gestation
• Diagnose with 2-step method
o 50gm one hour glucose challenge (<130 or <140)
o 100gm hour oral glucose tolerance test
What effect does altered glucose metabolism have on the fetus? Effect on mother? In order to
minimize fetal and maternal morbidity, what is the goal for glucose control in mothers diagnosed with
GDM?
• Goals of Insulin Therapy – compensate for decreased or inadequate endogenous insulin
o Fasting <95; Postprandial meals 1 hour <140 or 2 hours < 120
o Tight control decreases perinatal death, shoulder dystocia, fractures, and nerve palsy
• Fetus
o Excessive glucose transport to the fetus results in excessive fetal insulin and fetal growth
o Increase risk cesarean delivery, Erb’s palsy, clavicle fractures, fetal intolerance of labor and low Apgar scores
o Poor control DM – neonatal respiratory distress, cardiac septal hypertrophy, acidemia and hypoxia
• Neonate
o Hypoglycemia because neonate continues to produce increased insulin for first 24 hours, but neonate not experiencing
maternal hyperglycemia any more
o Hypercalcemia, Hyperbilirubinemia, Polycythemia (fetal response to hypoxia from hyperinsulinemia and increased O2
consumption leading to increased erythropoietin)
o Longterm effects – obesity, Type 2 DM
2
Summarize the types of hypoglycemic agents typically used to treat GDM and what is their mechanism
of action?
• Treatment is actually 3-legged stool approach: diet, exercise, medication
• Various forms of insulin differ in their onset and duration of action, allowing for more precise glucose control.
• Metformin and Glyburide cross the placenta, but insulin only in very high doses
Figures:
1. Fetal Effects of PreGestational Diabetes
2. Diabetogenic State
3. Human Placental Lactogen
4. Estrogen and Progesterone Effects
5. Pathophysiology of GDM
References:
• Beckmann, CRB, et al. Obstetrics and Gynecology. 8th edition. Baltimore, MD: Lippincott, Williams, and Wilkins, 2018.
• Caughey, AB and Turrentin, M. Gestational Diabetes Mellitus. ACOG Practice Bulletin Number 190, February 2018.
• Durnwald, C. Gestational diabetes mellitus: Glycemic control and maternal prognosis. Up to Date. July, 2018
• Kim, C and Ferrara A. Gestational Diabetes During and After Pregnancy. Springer-Verlag London Limited, 2010.